The choice for surgical repair depends on the person’s perception of their symptoms, and if they are interfering with quality of life at an unacceptable level. Most medical plans (whether private insurers or governmental healthcare entities) consider surgery to be a cosmetic procedure in most cases of DR. Surgery may be covered if specific criteria are met, including width, impact on activities of daily living, and evidence that the patient has done a trial of physical therapy for 6 months to a year with no discernable results. The specifics vary from country to country, so you may wish to do research depending on your locality.
The first line of treatment for diastasis recti is physical therapy for at least 6 months for good reason–the symptoms of diastasis recti are generally responsive to targeted exercises that strengthen the core,
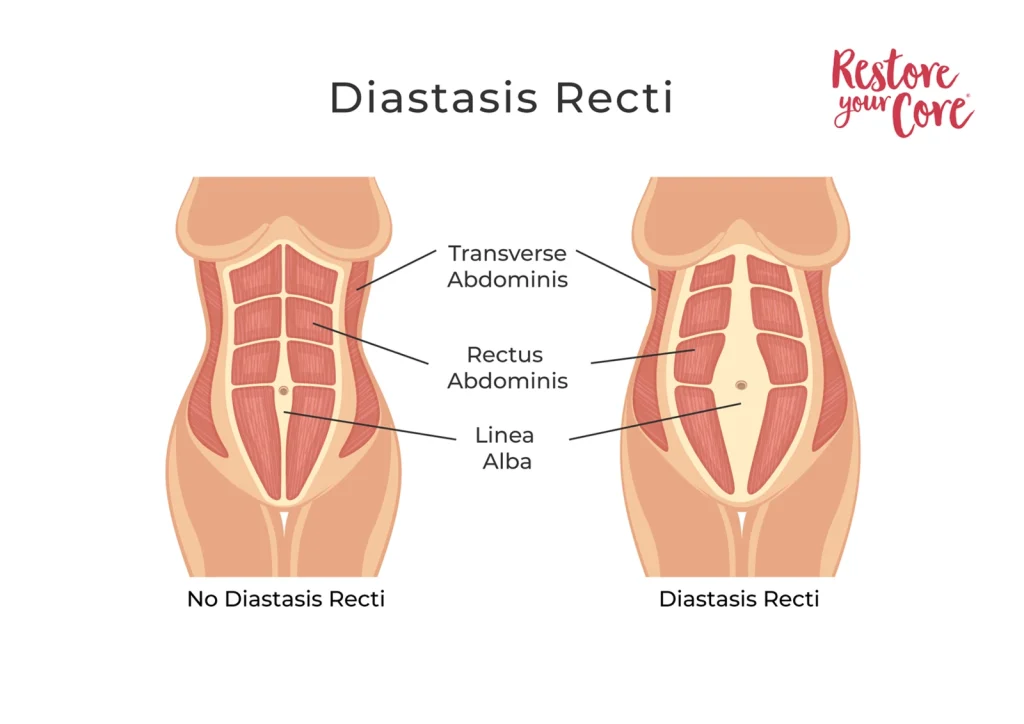
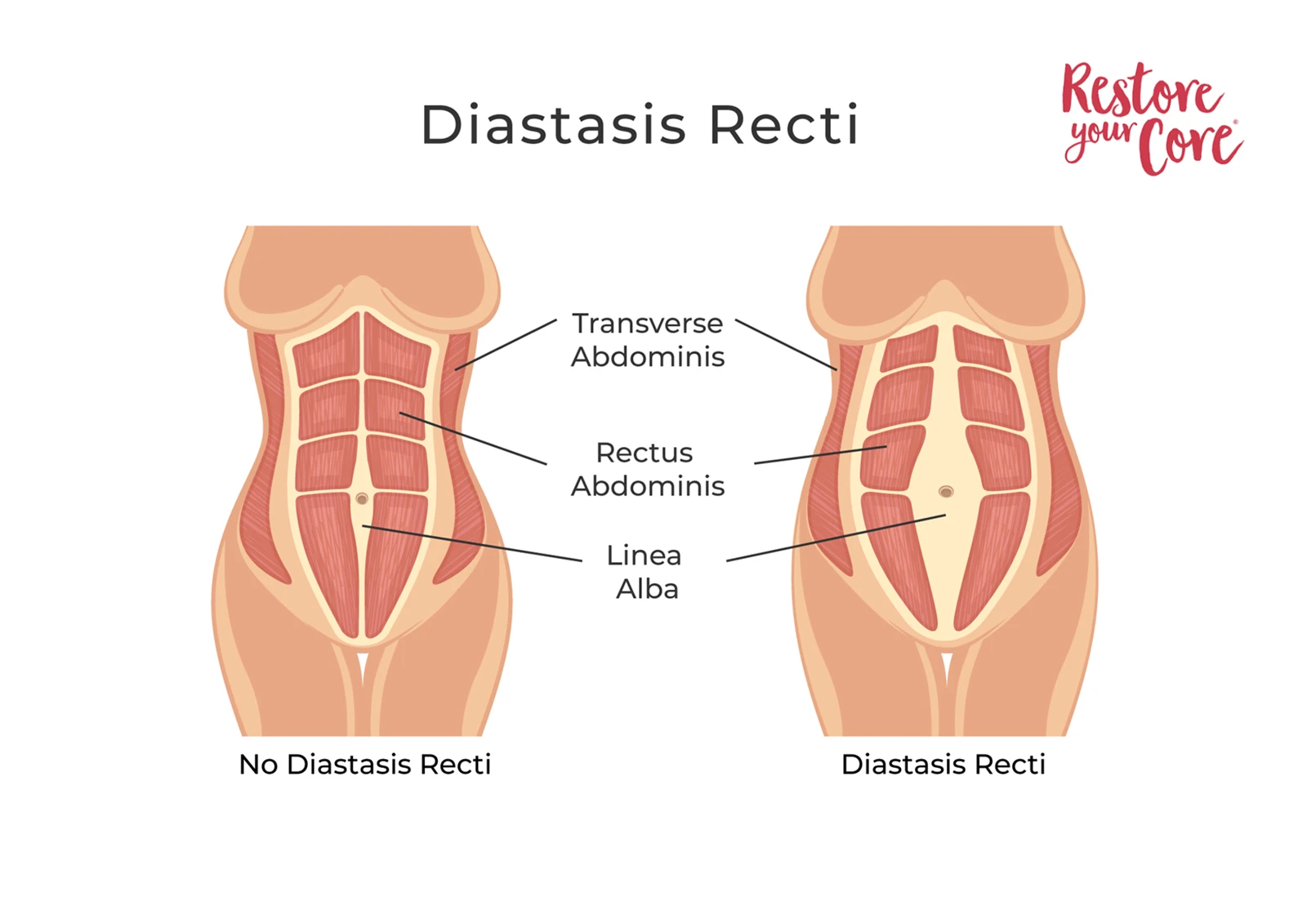
“[…] during the early post-natal period, exercises might be highly effective, making this a possible nonsurgical solution for DRA. Static abdominal contractions, pelvic rocking, sit-up and leg slide exercises are also recommended for a stubborn and protruding abdominal wall. Bilateral activation of the transversus abdominis can reportedly stabilize the ribs, linea alba and thoracolumbar fascia. Engaging the transversus abdominis shortens the rectus abdominis muscles and brings together the gap at the linea alba.
However, not all bodies respond equally well to exercise, and if a regular core-training regimen has been undertaken without success, there are several surgical routes that involve reducing the width of the stretched tissue of the linea alba” (Thabet, 2019).
Numerous studies have shown that there are few differences in terms of long-term outcomes among different types of surgical repair. One study indicates that incorporating core training both before and after surgery can significantly increase the overall effectiveness and long-term success of surgical outcome: “The study showed significant improvements in function. The self-reported symptoms of back pain, abdominal pain, core control, core weakness, bulging, constipation, urinary incontinence, and cosmetic issues showed significant improvements at the 1-year follow-up.
The two most common symptoms reported before surgery were back pain and lack of core control, and these also showed the greatest improvement at follow-up. Even though symptoms before and after surgery were registered as dichotomous yes/no answers, the findings reflect the panorama of functional disabilities reported in previous studies (Olsson et al., 2023).
In general, patient satisfaction is high with surgery, although, as Olsson et al. (2023) suggest, “The self-reported symptoms, bulging, and cosmetic issues significantly improved but remained to some extent. These ‘body image’ symptoms may need specially designed management. In cases with severe abdominal wall insufficiency, [rectus diastasis] repair alone may not be sufficient.” In other words, even if the DR is repaired, we need to keep in mind that body image issues can make a sense of “healing” difficult to access for some people.
While some cases of DR may require surgical intervention, the vast majority respond well to exercise. Non-surgical methods not only empower patients by making them feel strong and more capable physically but also have a well-documented positive impact on mental health.
Additionally, with adequate counseling and support around body image issues, individuals pursuing non-surgical methods often experience improvements in quality of life measures similar to those who undergo surgery.
How to fix diastasis recti without surgery?
There are a variety of approaches to healing diastasis recti without surgery, but all physical therapy and targeted exercise techniques will have in common a focus on better managing intra-abdominal pressure.
A comprehensive, holistic DR rehab protocol will include:
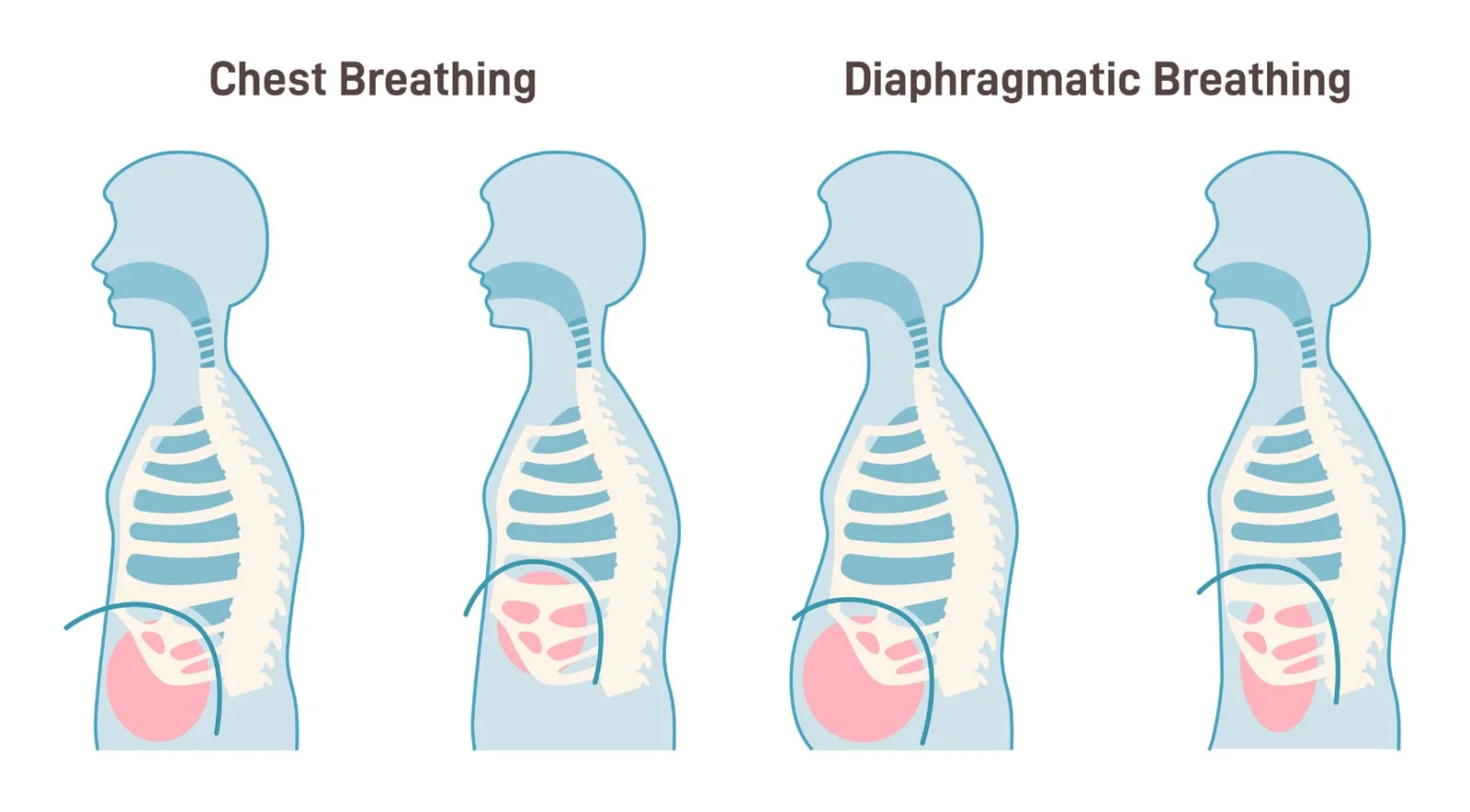
- A focus on establishing optimal breathing patterns, both relaxed and underload
- Exercises that help the patient learn to appropriately engage the core during movement, beginning with low load and progressively increasing
- Exercises integrating the transverse abdominal muscles with the other core musculature, including the rectus abdominis muscles
- Exercises that help patients increase the mobility and strength of the whole body, especially including shoulders, hips, and pelvic floor
- Coaching or counseling on relevant body image/mental health issues
It is surprisingly difficult to make an exhaustive list of exercises that have been shown through studies to effectively improve diastasis recti–there is no consensus in the literature. However, there is plenty of evidence that both practicing activation of the transverse abs and coordinating the use of the rectus abdominis with other muscle groups can have a positive effect on DR. Getting patients to train their core to be responsive to load requires giving plenty of opportunities for core engagement beyond supine exercises.
Your patients should look for providers or programs that offer a whole-body or holistic approach to diastasis recti healing. Exercise programs should be tailored to various stages of your patient’s recovery, with an emphasis on customization based on assessment. While most cases of diastasis recti have common aspects, each person’s body is unique and responds uniquely to exercise. Therefore, ongoing progress assessment is essential for effectively restoring core function.